

BREAKING NEWS
For the latest on Thailand Medical Industry, Thailand Doctors, Thailand Medical Research, Thailand Hospitals, Thailand Wellness Initiatives and the latest Medical News
The human heart has four valves which direct the flow of blood in the correct double-circulation mode, taking blood to and from the lungs as well as to and from the rest of the body. Two of the valves are on the right side and two on the left.
One pair of valves separates each lower chamber (atrium) from the upper chamber (ventricle), while the other pair separates the ventricles from the large blood vessels carrying blood away from the heart. The valve between the left atrium and ventricle is called the mitral valve and is composed of two fibrous leaflets covered with the same smooth endothelium as the rest of the heart’s interior. The leaflets are anchored to the wall of the heart by fibrous chords called the chordae tendinae.
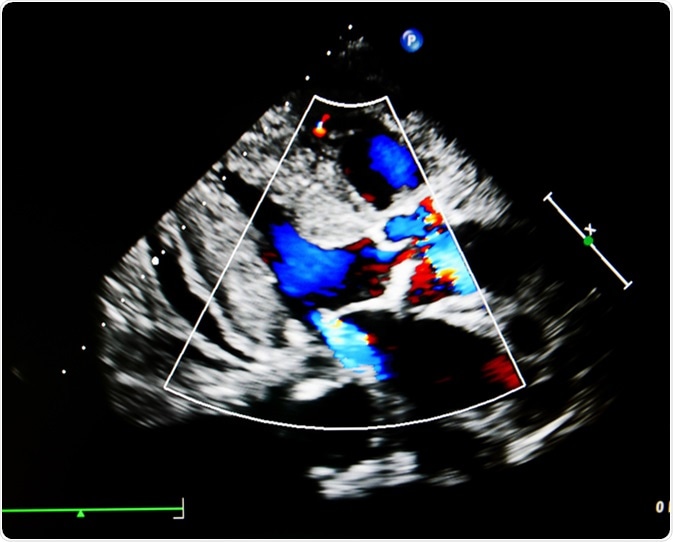
Mitral regurgitation (MR) is also called mitral insufficiency, and is a condition in which the valve allows blood to leak back into the left atrium when the ventricle contracts, instead of holding tight so that ventricular contractions can force blood out of the heart into the aorta, the great vessels that supplies branches to the various parts of the body except the lungs.
The causes of MR include primary and secondary conditions. Some of these include:
MR occurs more often in the following situations:
Mild MR is most often asymptomatic. As it progresses in some patients, it may produce symptoms such as:
Cardiac failure may occur because of severe regurgitation of blood into the left atrium, which leaks back again into the left ventricle when the heart relaxes. This progressively enlarges the left ventricle and weakens it, causing heart failure and lack of adequate circulation to the rest of the body. This leads to swelling of the lower limbs, weakness, shortness of breath and tiredness with mild exercise, among others.
The right side of the heart is also eventually affected because the left atrium is always filled with blood due to the leaky valve, and this prevents the proper emptying of blood coming in from the lungs to the left atrium, causing it to back up in the pulmonary circulation and eventually thickening the vessels in the lung. This forces the right side of the heart to pump harder to overcome this resistance, and it finally becomes weakened by overwork.
Cardiac arrhythmias, notably atrial fibrillation, because of the overstretching of the pacemaker region of the heart in the left atrium. This can cause clots to form in the heart because of the uncoordinated and weak contraction, which allows blood to pool in certain parts instead of flowing constantly. These clots may break off and travel to other blood vessels in the heart, lung and brain, causing strokes, heart attacks or pulmonary embolism.
The diagnosis of MR is made on clinical and imaging grounds. Management may include anticoagulants to prevent clots in the heart, but in severe cases or sudden onset of MR, surgery is required to repair or replace the faulty valve with artificial mechanical or bioprosthetic valves.