Study Shows That New York’s SARS-CoV-2 Variant Also Known As The Iota Or B.1.526 Variant Increases The Risk Of Mortality In Older Adults
Source: SARS-Co-2 Iota Variant Aug 13, 2021 4 years, 11 months, 1 day, 7 hours, 39 minutes ago
Iota Variant: Alarmingly, a new study by researchers from Columbia University and the New York City Department of Health and Mental Hygiene has found that the SARS-CoV-2 B.1.526 variant increased the risk of mortality for older adults who contracted the virus.

The study also determined the transmission rate, immune escape ability, and infection fatality rate of the B.1.526 variant.
The study findings revealed that the variant has considerably higher transmissibility and immune escape potential than previously circulating variants and that it can increase the infection fatality rate by 62% - 82% among older adults.
The study team utilized nine epidemiological and population datasets collected in New York City (NYC), where B.1.526 emerged, and comprehensive modeling to estimate the changes in transmissibility, immune escape potential, and infection fatality risk (IFR) for B.1.526.
The study findings showed that the estimated transmission rate in the neighborhood where B.1.526 was initially detected was consistently higher than other neighborhoods in NYC and further increased during the weeks preceding B.1.526 detection, likely due to its early spread there. Overall, models estimated that B.1.526 had transmissibility about 15-25% higher than previously circulating variants and that it could escape immunity in 0-10% of previously infected persons. In addition, B.1.526 substantially increased IFR in older adults: by 46% (95% CI: 7.4 – 84%) among 45-64 year-olds, 82% (95% CI: 20 – 140%) among 65-74 year-olds, and 62% (95% CI: 45 – 80%) among 75+ during Nov 2020 – Apr 2021, compared to baseline IFR estimated for preexisting variants.
The study findings were published on a preprint server and are currently being peer reviewed.
https://www.medrxiv.org/content/10.1101/2021.08.04.21261596v1
As the COVID-19 pandemic progresses, several new variants of SARS-CoV-2 have been identified. Because of increased infectivity and pathogenicity, some of these variants have been designated as Variants of Concern (VOC) or Variants of Interest (VOI) by the World Health Organization (WHO).
The new B.1.526 variant of SARS-CoV-2, also known as the
Iota variant, was first identified in New York City in November 2020.
The Iota variant has two notable mutations: the E484K spike mutation, which may help the virus evade antibodies, and the S477N mutation, which may help the virus bind more tightly to human cells. The Iota (B.1.526) genome also contains the following amino-acid mutations, all of which are in the virus's spike protein code: L5F, T95I, D253G, E484K, D614G and A701V.
To date the variant has been detected in all 52 states in the United States, as well as in 29 countries across the world including countries in South-East Asia.
Laboratory based observational studies revealed that this variant is modestly resistant to neutralization by therapeutic monoclonal antibodies and vaccine/infection-induced antibodies.
There is still not much data as to whether this new va
riant increases or decreases the risk of breakthrough infections in vaccinated or previously infected individuals.
The study team had analyzed multiple epidemiological and population datasets collected in New York City and performed mathematical modeling to determine the transmission rate, immune evasion ability, and infection fatality risk of the B.1.526 variant.
The team utilized a network model-inference system to estimate the transmission dynamics of SARS-CoV-2 and population-level variables and parameters in New York City. Based on collected information, they conducted a city-level multi-variant, age-structured modeling analysis to estimate the infection and immune evasion ability changes for the B.1.526 variant. The final analysis utilized the data obtained from two models to estimate the variant-specific mortality rate among individuals infected with SARS-CoV-2 (infection fatality risk).
Also for the network model-inference system, they utilized multiple epidemiological datasets as well as vaccination datasets.
Similarly, the multi-variant model analysis utilized four weekly datasets, including confirmed and suspected COVID-19 cases, hospitalizations, mortality, and percentage of different SARS-CoV-2 variants circulating in New York City.
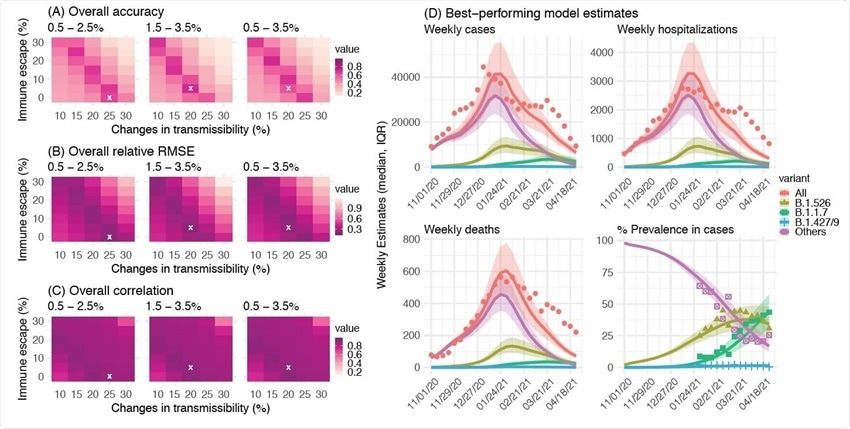 Detailed comparison of different combinations of changes in transmissibility and immune escape property for B.1.526. Left panel shows the overall accuracy (A), relative RMSE (B), and correlation (C) of model estimates under different transmissibility and immune escape settings. White crosses (x) indicate the best-performing parameter combination. Right panel shows model estimates using the overall best-performing parameter combination (i.e., 1.5-3.5% initial prevalence, 15-25% higher transmissibility, and 0-10% immune escape). Lines and surrounding areas show model-simulated median estimates and interquartile range; dots show corresponding observations; colors indicate different variants as specified in the legend. Note that these model simulations used same infection-detection rate, hospitalization-rate and IFR (i.e., average during Nov 2020 – Apr 2021); that is, they did not account for changes in case ascertainment or disease severity by week during this period, due to, e.g., increases in disease severity by the new variants. As such, there were larger deviations from the observations during later months of the simulation with more infections by the new variants.
Detailed comparison of different combinations of changes in transmissibility and immune escape property for B.1.526. Left panel shows the overall accuracy (A), relative RMSE (B), and correlation (C) of model estimates under different transmissibility and immune escape settings. White crosses (x) indicate the best-performing parameter combination. Right panel shows model estimates using the overall best-performing parameter combination (i.e., 1.5-3.5% initial prevalence, 15-25% higher transmissibility, and 0-10% immune escape). Lines and surrounding areas show model-simulated median estimates and interquartile range; dots show corresponding observations; colors indicate different variants as specified in the legend. Note that these model simulations used same infection-detection rate, hospitalization-rate and IFR (i.e., average during Nov 2020 – Apr 2021); that is, they did not account for changes in case ascertainment or disease severity by week during this period, due to, e.g., increases in disease severity by the new variants. As such, there were larger deviations from the observations during later months of the simulation with more infections by the new variants.
Importantly in New York City, the population-level prevalence of SARS-CoV-2 infection was estimated to be 16.6% at the end of the first pandemic wave.
However at the end of the second wave, the estimated prevalence was 41.7%.
Although most SARS-Cov-2 infections occurred in the older population during the first wave, the second wave caused infections in all age groups.
Interestingly a rapid increase in B.1.526-infected cases was observed during the second pandemic wave. Before the identification of the variant in a specific neighborhood for the first time in early November 2020, a gradual increase in the overall SARS-CoV-2 transmission rate was observed in the same neighborhood.
The transmission rate remained high between November 2020 and February 2021, followed by a reduction to the baseline when the B.1.526 variant became dominant across the city.
However in contrast, the transmission rate remained constant in other neighborhoods. Overall, these observations indicate that the rise in transmission rate in that particular neighborhood is probably due to the early rapid spread of the B.1.526 variant.
Interestingly the estimation made from the collected data revealed that the transmission rate of the B.1.526 variant is 15-25% higher than that of previously circulating variants.
Also significantly, the data revealed that the variant can induce breakthrough infections in 0-10% of the population. With this moderate increase in transmissibility and immune evasion ability, the B.1.526 variant became dominant in New York City from November 2020 to March 2021. Afterward, with the surge of more infectious variant B.1.1.7, the prevalence of B.1.526 variant decreased gradually.
Alarmingly despite a reduction in mortality rate following mass vaccination, an induction in infection fatality rate was estimated in New York City during the second pandemic wave.
This estimations made by the study team about variant-specific infection and mortality rates revealed that the B.1.526 variant increases the infection fatality rates by 46%, 82%, and 62% in individuals aged 45-64 years, 65-74 years, and above 75 years, respectively.
Compared to previously circulating variants, the B.1.526 variant, overall, caused a 60% induction in the infection fatality rate. This induction was comparable to that estimated for the B.1.1.7 variant.
The findings highlight the importance of monitoring the epidemiological characteristics of novel SARS-CoV-2 variants to better manage the COVID-19 pandemic.
For more about the
Iota Variant, keep on logging to Thailand Medical News.





























